This guide provides a comprehensive overview of Tirzepatide, a dual-action therapeutic designed for metabolic health, glycemic control, and weight management.
Classification & Nature
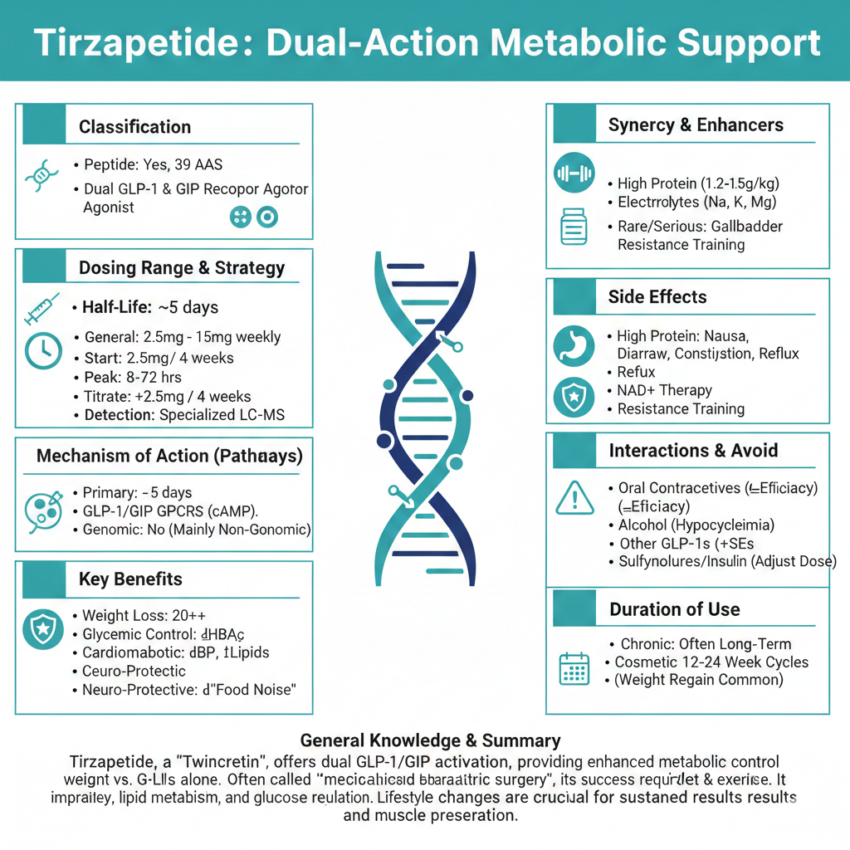
- Peptide: Yes, it is a synthetic, acylated peptide (a chain of 39 amino acids).
- Classification: Dual GLP-1 (Glucagon-like peptide-1) and GIP (Glucose-dependent insulinotropic polypeptide) receptor agonist.
Dosing Range & Strategies
- General Range: 2.5 mg to 15 mg per week.
- Loading/Starter Dose: 2.5 mg once weekly for the first 4 weeks (primarily to assess tolerability).
- Titration Strategy: Increase by 2.5 mg every 4 weeks until the target dose or maximum tolerable dose (15 mg) is reached.
- Maintenance: Once target weight/glucose levels are reached, users often stabilize at their effective dose (e.g., 5 mg, 10 mg, or 15 mg).
Pharmacokinetics & Saturation
- Half-Life: Approximately 5 days.
- Time to Peak: 8 to 72 hours after injection.
- Peak Saturation: Steady-state levels are typically reached after 4 weeks of consistent dosing.
- Detection: Not tested in standard 5-panel or 10-panel drug screens; requires specialized liquid chromatography-mass spectrometry (LC-MS) for detection.
Mechanism of Action (Pathways)
- Primary Pathways: Stimulates both GLP-1 and GIP receptors.
- Genomic vs. Non-Genomic: Primarily Non-Genomic. It works through cell-surface G-protein coupled receptors (GPCRs) to trigger rapid intracellular signaling (cAMP pathway), though long-term use can lead to genomic changes in gene expression related to insulin secretion and cell preservation.
Key Benefits
- Weight Loss: Significant reduction in body fat (up to 20%+ in clinical trials).
- Glycemic Control: Lowers HbA1c and improves fasting/postprandial glucose.
- Cardiometabolic: Improves blood pressure, lipid profiles, and reduces systemic inflammation (CRP).
- Neuro-Protective: Potential benefits in reducing “food noise” and addictive cravings.
Synergy & Performance Enhancers
- High Protein Intake: Essential (1.2g–1.5g per kg) to prevent muscle wasting (sarcopenia) during rapid fat loss.
- Electrolytes: Sodium, Potassium, and Magnesium help mitigate the “keto-like” fatigue and headaches.
- NAD+ Therapy: Often used concurrently to boost mitochondrial energy and metabolic rate.
- Resistance Training: Crucial to maintain lean mass and bone density.
Side Effects
- Gastrointestinal: Nausea, vomiting, diarrhea, constipation, and acid reflux (most common).
- Injection Site: Redness, itching, or minor swelling.
- Serious (Rare): Pancreatitis, gallbladder issues, and theoretical risk of thyroid C-cell tumors.
Interactions & Things to Avoid
- Oral Contraceptives: Tirzepatide slows gastric emptying, which may reduce the absorption and efficacy of oral birth control.
- Alcohol: Can increase the risk of hypoglycemia and severe dehydration.
- Other GLP-1s: Do not stack with Semaglutide (Ozempic/Wegovy) or Liraglutide, as they target the same pathways and increase side effect risks.
- Sulfonylureas/Insulin: May require dose reduction of these medications to avoid dangerously low blood sugar.
Duration of Use
- Chronic Management: Often intended for long-term or indefinite use for chronic obesity/T2DM management.
- Cycle Duration: If used for cosmetic weight loss, “cycles” typically last 12–24 weeks, though weight regain is common if lifestyle changes are not maintained post-cessation.
General Notes:
Tirzepatide represents a significant evolution in metabolic medicine. While its predecessor, Semaglutide, focuses solely on the GLP-1 receptor, Tirzepatide’s “Twincretin” approach adds GIP receptor activation. This secondary pathway is thought to better manage the way the body handles fat (lipids) and may reduce some of the nausea associated with GLP-1-only drugs, allowing for higher, more effective dosing.
Clinically, Tirzepatide is often described as “medical bariatric surgery” due to its profound impact on satiety and metabolic flexibility. However, it is not a “magic bullet.” Success is heavily dependent on maintaining a nutrient-dense diet and consistent resistance training to ensure the weight lost is predominantly fat rather than vital muscle tissue.