Understanding the Challenge and Restoring Balance
The use of Performance-Enhancing Drugs (PEDs), specifically anabolic-androgenic steroids (AAS), by females can lead to a condition known as virilization, or masculinization. This involves the development of male secondary sexual characteristics due to an imbalance of androgens (male hormones) versus estrogens and progesterone (female hormones).
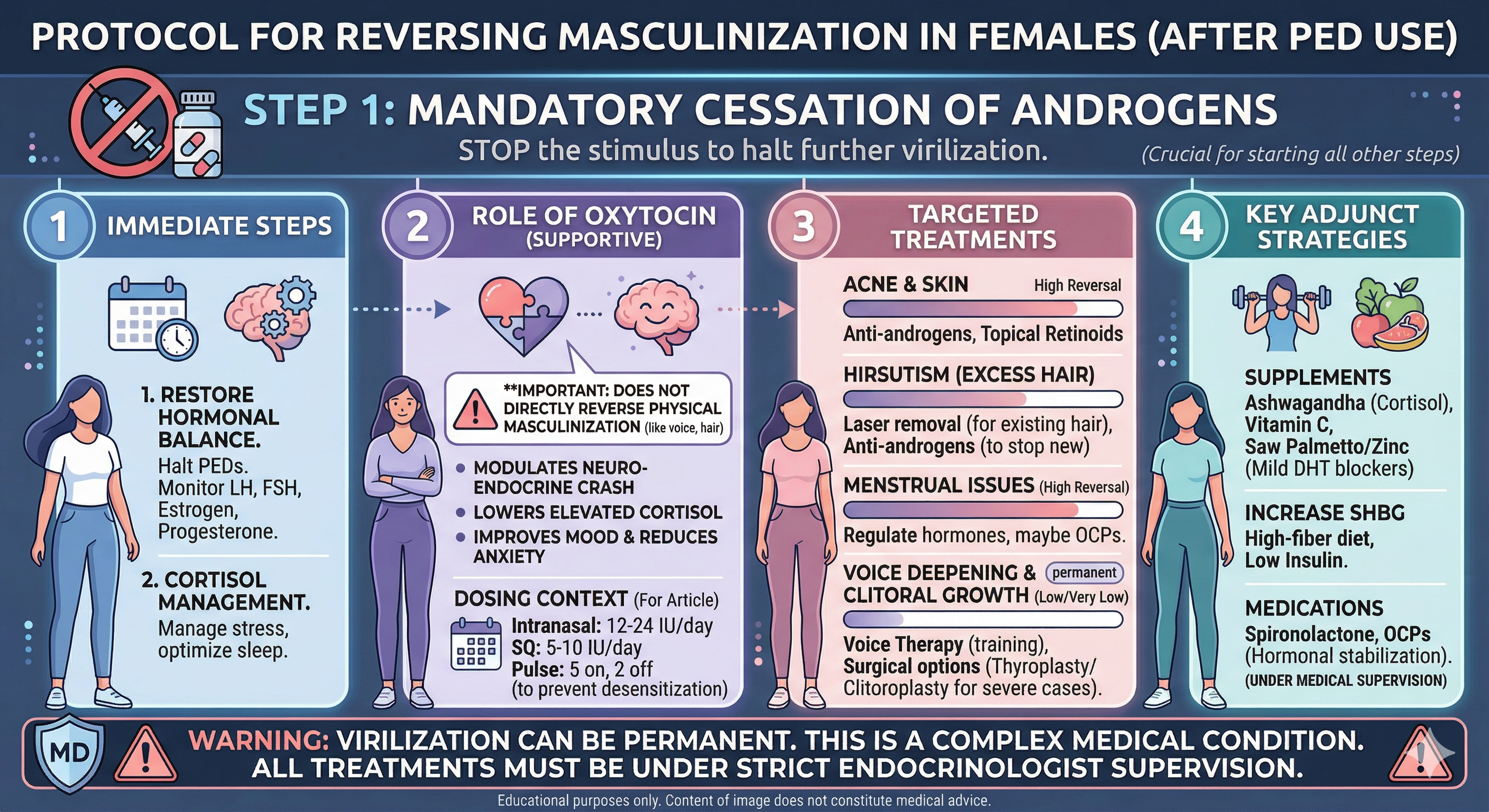
While some of these changes are reversible once the offending substance is removed, others can be long-lasting or even permanent. This article provides a comprehensive overview of a structured protocol for reversing masculinization, covering mandatory medical steps, supportive supplements, prescribed medications, and specialized therapies.
Step 1: Immediate Cessation (Non-Negotiable)
The absolute first step in any reversal protocol is the immediate and complete discontinuation of the PEDs. Continuing to use these substances while attempting a reversal is counterproductive and will worsen the condition.
Step 2: Medical Oversight and Hormonal Restoration
Virilization is a serious medical condition that requires the guidance of a qualified healthcare professional, ideally an endocrinologist with experience in hormone-based therapies. Self-treating can be dangerous.
The Role of Oxytocin
Oxytocin is sometimes included in reversal protocols, though its role is more supportive than corrective for physical virilization.
- Anti-Glucocorticoid Effects: Oxytocin may help lower systemic cortisol, which is often elevated during and after PED cycles. High cortisol can exacerbate skin issues and metabolic stress.
- Mood and Neuroprotection: It can help mitigate the “crash” associated with ending a cycle, potentially reducing irritability or depressive symptoms by acting on the brain’s reward and social bonding centers.
- Caveat: There is no clinical evidence that oxytocin directly reverses physical virilization like voice deepening or hair growth.
As mentioned, oxytocin is a hormone often discussed for its supportive role in these protocols.
- Potential Mechanisms: While not a direct anti-androgen, oxytocin may offer neuroprotective benefits, helping to mitigate the mood fluctuations and cognitive “crash” often experienced when ending a steroid cycle. It might also modulate certain stress pathways that can worsen skin conditions like acne.
- Scientific Caveat: It is crucial to understand that there is no scientific evidence suggesting oxytocin can directly reverse physical virilizing changes like voice deepening or clitoral enlargement. It is used as a supportive adjunct, not a primary corrective agent for physical virilization.
Dosing Strategies for Oxytocin
Oxytocin is typically administered via intranasal spray or subcutaneous (SQ) injection. The nasal route is often preferred for its direct access to the brain via the olfactory pathway, while SQ injections provide more systemic stability.
1. Intranasal Administration (Common)
This is the most frequent method for mood regulation and “resetting” the HPA axis.
- Standard Dose: 12 IU to 24 IU (International Units).
- Frequency: Once or twice daily (e.g., once in the morning and once before bed).
- Protocol Length: Often used for 2–4 weeks during the acute withdrawal phase from PEDs.
2. Subcutaneous (SQ) Injection
Used when a more consistent systemic level is desired to manage high cortisol or metabolic stress.
- Standard Dose: 5 IU to 10 IU (approx. 10mcg to 20mcg).
- Frequency: Once daily, usually in the evening to assist with sleep and recovery.
- Note: This method has a higher impact on physical receptors (like those in the uterus or breasts).
Critical Considerations for Females
When building a protocol specifically for women, there are unique physiological risks to account for:
The “Uterine” Factor
Oxytocin’s primary medical use is inducing labor. In a non-pregnant female:
- Cramping: Higher doses (especially via SQ injection) can cause significant uterine contractions and pelvic discomfort.
- Timing: It is often best to avoid high-dose oxytocin during the menstrual window to prevent exacerbating cramps.
Water Retention (Vasopressin-like Effect)
Oxytocin is structurally similar to Vasopressin (ADH). At high or frequent doses, it can cause the body to retain water and lower sodium levels (hyponatremia).
- Strategy: Maintain adequate electrolyte intake and monitor for sudden “puffiness” or headaches.
Desensitization
The body can downregulate oxytocin receptors if they are overstimulated.
- Strategy: Use a “5 days on, 2 days off” schedule or limit use to the first 21 days of the reversal protocol to maintain sensitivity.
Summary Table for the Article
| Method | Typical Dose | Primary Benefit |
| Intranasal Spray | 12–24 IU Daily | Brain-targeted; improves mood and lowers anxiety. |
| SQ Injection | 5–10 IU Daily | Systemic; aids in cortisol management and sleep. |
| Pulsed Dosing | 5 days on / 2 off | Prevents receptor desensitization. |
Step 3: Targeted Interventions (Supplements, Drugs, and Therapies)
The protocol must be tailored to the specific symptoms, as their potential for reversal varies significantly.
| Symptom | Reversal Potential | Primary Intervention |
| Acne & Oily Skin | High | Topical retinoids, oral antibiotics (if needed), hormonal stabilization. |
| Hirsutism (Excess Body/Facial Hair) | Moderate/High (Gradual) | Anti-androgens, cosmetic therapies. |
| Menstrual Irregularities | High (Once HPO axis recovers) | Hormonal stabilization, potential use of oral contraceptives. |
| Clitoral Enlargement (Clitoromegaly) | Low/Partial (Slight regression possible) | Time and androgen cessation; severe cases require surgery. |
| Voice Deepening (Dysphonia) | Very Low/Permanent | Voice training/therapy; thyroplasty (surgery). |
Comprehensive Treatment Modalities
1. Nutritional Supplements (Supportive Role)
Supplements can support the body’s natural endocrine recovery and manage symptoms like high cortisol.
- Supplements to Lower Cortisol & Support Mood:
- Ashwagandha: An adaptogenic herb that may help lower systemic cortisol and support mood stability during the “crash.”
- Vitamin C: Supports the adrenal glands and may modulate the stress response.
- Supplements to Boost SHBG:
- Increasing SHBG (Sex Hormone-Binding Globulin) is beneficial as it binds to free androgens (testosterone, DHT), making them inactive.
- High-Fiber Diet & Low Insulin: While not a supplement, managing insulin levels through diet can increase SHBG levels.
- Targeted DHT Support (for Hair Loss):
- Saw Palmetto & Zinc: These are often used as mild, natural 5-alpha reductase inhibitors to reduce the conversion of testosterone to DHT (dihydrotestosterone), which is primarily responsible for androgenic hair loss and hirsutism.
2. Prescribed Medications (Corrective Role)
Medical intervention is often necessary to actively counter the high androgen levels and their systemic effects.
- Anti-Androgens:
- Spironolactone: This is a diuretic with potent anti-androgenic properties. It competes with androgens for binding sites on the androgen receptor and can reduce androgen production. It is highly effective for acne and hirsutism but must be monitored for its effects on potassium levels.
- 5-Alpha Reductase Inhibitors (for Hirsutism/Hair Loss):
- Finasteride (or Dutasteride): These drugs inhibit the enzyme 5-alpha reductase, significantly lowering DHT levels. They can slow hair loss and, combined with anti-androgens, reduce excess body hair growth. (Crucial Note: These medications are strictly contraindicated in women who are pregnant or planning to become pregnant due to the risk of severe birth defects in male fetuses).
- Hormonal Stabilization:
- Oral Contraceptive Pills (OCPs): Combined OCPs (containing estrogen and progestin) suppress LH and FSH, thereby reducing the ovaries’ production of androgens. They also increase SHBG, further lowering free androgen levels. This can help regulate the menstrual cycle and improve acne.
3. Specialized Therapies (Structural Changes)
Symptoms that involve structural changes to the body often require non-pharmaceutical interventions.
- Vocal Changes (Deepening):
- Voice Training/Speech Therapy: A speech-language pathologist specializing in vocal feminization can help women learn techniques to alter their vocal resonance, pitch, and intonation, maximizing the use of their remaining vocal range.
- Thyroplasty (Surgery): If vocal changes are severe and do not respond sufficiently to therapy, surgical procedures can modify the laryngeal structure to permanently raise vocal pitch.
- Clitoral Enlargement:
- Clitoroplasty (Surgery): This is a specialized surgical procedure to reduce the size of the clitoris while preserving sensation. It is usually reserved for severe cases of clitoromegaly.
- Cosmetic Therapies (for Hirsutism):
- Laser Hair Removal & Electrolysis: While medications can stop new male-pattern hair growth, they rarely eliminate existing terminal hairs. Laser therapy and electrolysis are necessary to permanently remove the hair that has already developed.
The Road Ahead: Patience and Care
The journey of reversing masculinization is often slow and requires a multi-pronged strategy. While some symptoms will resolve relatively quickly once the body’s hormonal balance is restored, others are a testament to the powerful, long-lasting nature of androgens on the female physiology. Commitment to a medically supervised protocol, lifestyle adjustments, and perhaps the utilization of specialized therapies can offer the best chance for reversion.